
Manifesto for Agentic Commercialization
What if we could slash 90% of the costs of bringing a new therapy to market?

AI is quickly reshaping the commercialization model in life sciences. There’s a multi-billion-dollar opportunity for pharma and emerging biotech to bring clinical-stage therapies to market faster, more efficiently, and with better execution—by combining human expertise with trustworthy Agentic AI.
McKinsey estimates generative AI could unlock $60–110 billion in annual value across pharma and medical products, with $18–30 billion in commercial functions alone1; the AI-in-pharma market is forecast to grow roughly nine-fold this decade2; and the pharmaceutical-marketing market already exceeds $30 billion a year3, with the majority of this work outsourced to agencies.
Agentic Commercialization is how the industry will achieve these major wins for patient outcomes. But first, we need to cover some ground:
Why Now?
Why Trust?
The Vision
How We Get There
The Invitation
Why Now?
What makes this moment unique and ripe for disruption? Three forces are converging at once:
AI is rewriting how commercialization work gets done
Generative and agentic AI are moving from experiment to operating lever. Commercial is now the second-highest gen-AI priority in life sciences after research, and the work most exposed is exactly the high-cognitive, agency-driven work upstream of launch: McKinsey notes that pharma’s creative and content-production process is today “almost completely outsourced” to agencies4—and is now moving in-house as AI absorbs drafting work.
Launch economics are punishing—and getting worse
Bringing a drug from discovery to launch now costs about $2.7 billion, including the cost of failure.5 Yet roughly two-thirds of launches miss their first-year forecasts, and more than half generate under 80% of expected sales.6 Only about one in ten recent launches cleared $100 million in year one—half the prior rate—and a ZS retrospective found that commercial commitment, not the molecule alone, lifts a launch’s overperformance rate from 49% to 67%.7 Execution is the variable that decides outcomes, and the window to get it right is short.
Trust—not model capability—is the real barrier
The bottleneck to scaling AI in this industry is trust. An estimated 95% of enterprise AI pilots fail to deliver measurable business impact,8 even as 72% of CEOs report board pressure to show AI outcomes.9 In a regulated market, capability without compliance does not get adopted.
Why Trust?
We’ve entered a world where patients and healthcare providers (HCPs) get much of their clinical information self-serve from Large Language Model (LLM)-based assistants—ChatGPT, OpenEvidence—and less often from field teams and pharma companies. Two critical developments flow from that:
First, this means brands have influence over their clinical message, but not control. These models are non-deterministic, so while pharma companies can shape the inputs that go into LLMs, they can’t dictate the output. While this was already somewhat the case with HQ unable to control exactly what comes out of a sales rep or MSL’s mouth in a hall call, LLMs have made control over the clinical message even more difficult than before.
Second, information asymmetry is collapsing fast. HCPs used to rely primarily on pharma companies for treatment information because they had no other preferred way to get it—no searchable internet, no synthesis tool. That gap is closing. OpenEvidence can scrape the sources and synthesize the latest clinical data as well as, or faster than, a company can push it out.
So the real question becomes: in a world of democratized information, how does a brand create value? How do you differentiate when clinical information delivery is no longer scarce and valuable to HCPs?
The answer isn’t more information. It’s human connection—helping HCPs think through that knowledge and apply it to the patient in front of them.
For example, take a rare disease like narcolepsy. Knowing the textbook symptoms and pulling the latest research resources isn’t the hard part—an LLM can list them within seconds. The hard part is pattern-matching those symptoms to the actual patient sitting in your office, when fatigue could point a dozen different directions. That’s where a rep who knows the patients in a doctor’s practice—not just the drug—becomes genuinely useful: not competing with the chatbot on knowledge, but being a trusted partner to help the HCP apply it.
The role of field teams will continue to shift away from information delivery towards more strategic partnership and relationship building with the HCP. But the bedrock of this evolving relationship is trust.
The Vision
Bringing a therapy to market can require hundreds of millions to billions of dollars, and engaging payers, providers, and patients in an increasingly competitive market is hard. The goal is not to cut the customer-facing human roles that educate the market and build trust. AI’s jaggedness10 means that though AI will become superhuman in many areas, there will remain skills and competencies that remain uniquely human: connection, strategy, and judgment.
The goal is to remove waste in upstream work while making downstream, customer-facing teams more effective.
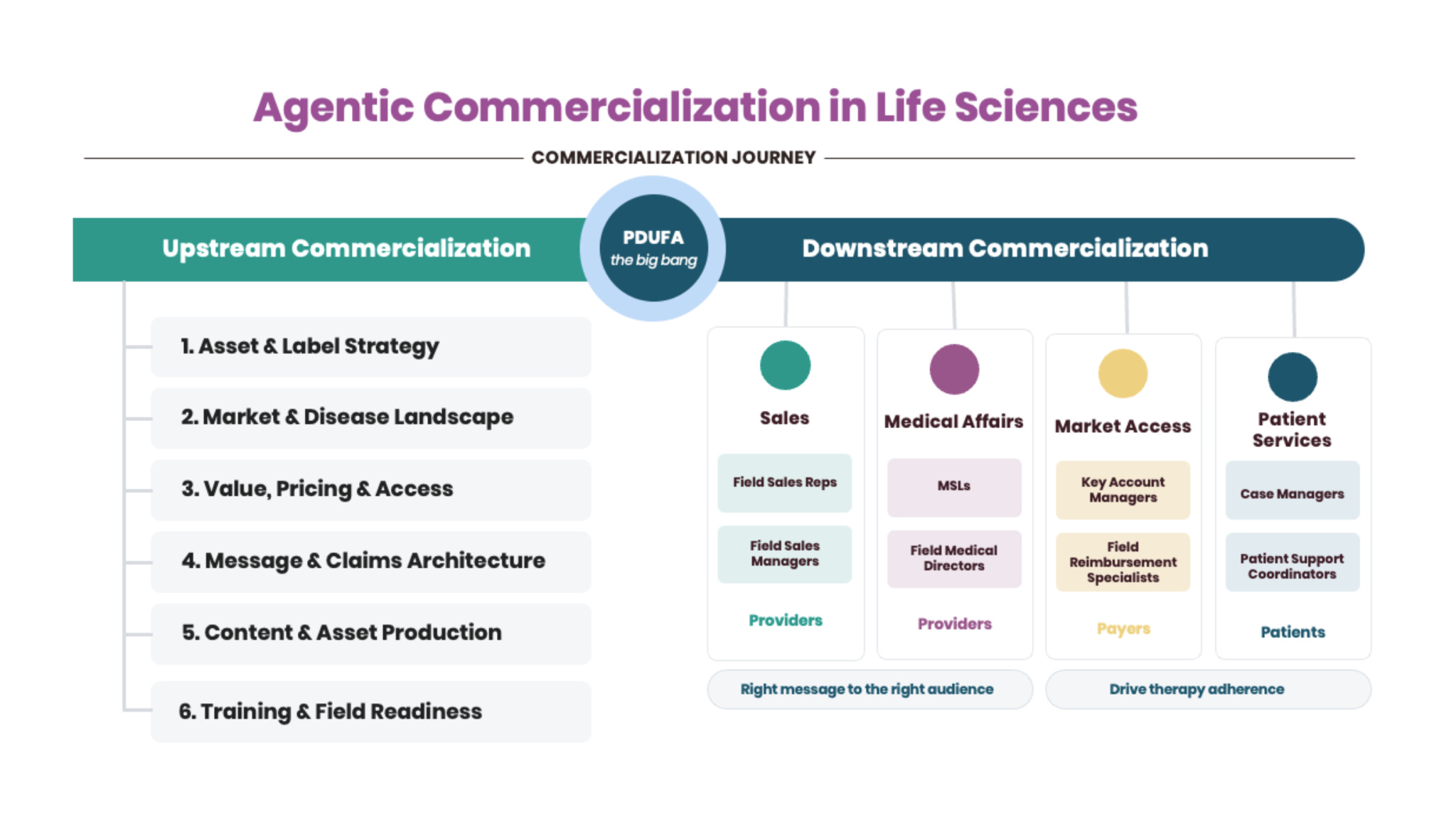
Life sciences commercialization has two zones:
Upstream commercialization—the efficiency opportunity
The high-cognitive, strategic work that happens before and around launch: launch readiness, message and claims architecture, market-access planning, content development, training curriculum, patient-services design, and insight synthesis. Today much of this is outsourced to agencies and consultants at very high cost — still produced through PowerPoints, manual workshops, and expensive human labor. The goal here is efficiency.
Downstream commercialization—the effectiveness opportunity
The strategy is set, the message is defined, and territories, customers, payer plans, and launch plans are in motion; now the company needs its human teams — medical affairs, sales, market access, and patient services—to execute well. The goal here is effectiveness.
In one line: upstream, make expensive commercialization work faster and cheaper; downstream, make the humans who engage customers better.
With agentic commercialization, pharma companies could slash the cost of getting a therapy to the patients who need it to one-tenth of what it is today—from $2.7 billion to as little as $277 million. It sounds audacious, yes. But imagine if upstream, pharma companies could bring institutional knowledge back in-house and agentify this high-cognitive, strategic work, saving millions. And then imagine downstream, if field teams had 40% of their day back12 to focus on high-value work, how that would transform and sharpen each field interaction. Then expand that time saved across every customer-facing touchpoint of a launch.
The MSL, freed from the busywork of writeback notes, is able to show up fully in the conversation with an HCP because he’s not thinking about all the admin work he has to do after. The Patient Support Coordinator catches a reimbursement denial before it becomes a three-month gap in a patient’s therapy, instead of after. And most importantly, the patient receives the therapy not eighteen months after approval, but now.
How We Get There
The central currency in Agentic Commercialization is trust, and trust has two inseparable parts: Compliance and Capability.
Here is the core equation: Trust = Compliance + Capability.
An agent that is compliant but not capable is useless—think of every voice assistant you don’t bother asking anything because you know its scope is limited. An agent that is capable but not compliant is dangerous, especially in the life sciences industry. They’re like a brilliant intern with no instinct for what they’re allowed to say.
In this industry, patient outcomes are at stake, so the cost of non-compliance is not symmetric with the upside of capability. Raw capability on its own is disqualifying.
Where an agent sits in terms of role decides which force has to lead. For front line teams interacting with providers, payers and patients, compliance leads to ensure consistency and control. For strategy, capability leads for higher quality insight. Upstream roles need a thought partner operating at the edge of human cognition. Downstream roles need an execution partner. For example, a CMO ideating with their team on GTM strategy and messaging has more berth to soundboard a vast array of ideas, whereas a sales rep needs to stick to the clinical message.
Every agent is really a coordinate defined by who it serves in the organization and where it sits in the commercialization timeline. There is no one-size-fits-all approach to this, but there is major potential upside.
Large incumbents—Veeva, Salesforce, IQVIA, Axtria, ZS, and the agency networks—each own parts of the pre-agentic commercialization journey, but they must re-earn credibility in the agentic-first categories now emerging, and they carry the inertia of existing portfolios and cultures. New AI-native entrants move fast but lack the domain depth, master agreements, and brand equity this market demands. The winning formula lies somewhere in the middle: companies that are small and innovative enough to make AI-native bets, but also fluent in the workflows, compliance constraints, personas, and change-management realities of life sciences commercialization.
The Invitation
If any of this resonates, I invite you to follow along. This is what The Agentic Dose is about: a space for pharma CEOs, biotech founders, and their investors to define what commercialization becomes next.
Over the next few months, we’ll unpack how agentic commercialization can drive effectiveness downstream for each functional area: Commercial L&D, Medical Affairs, Field Sales, Market Access, and Patient Services. We’ll then move upstream into the strategic work behind Brand & Marketing, Sales, Medical Affairs, Market Access, and Patient Services.
I’ll be thinking through the hard parts of making this vision a reality—the architecture, the failures, and the questions I don’t yet have answers to.
Let’s bring this vision to bear. Together.
References & Footnotes
1 McKinsey Global Institute estimates generative AI could create $60–110 billion in annual value for the pharmaceutical and medical-products industries, including $18–30 billion in commercial functions alone. McKinsey & Company, 2023–2024.
2 AI in the pharmaceutical market is projected to grow from ~$1.9 billion (2025) to ~$16.5 billion (2034), a ~27% CAGR. Precedence Research, 2025.
3 The pharmaceutical-marketing market is estimated at ~$31 billion (2025), reaching ~$56 billion by 2032. Research and Markets, 2026.
4 McKinsey observes that pharma marketing’s creative and production process is today “almost completely outsourced” to agencies. McKinsey & Company, 2024.
5 Average cost to advance a drug from discovery to launch reached ~$2.67 billion in 2025 (up from ~$2.23 billion in 2024), including the cost of failure. Deloitte, “Measuring the return from pharmaceutical innovation,” 2025.
6 Roughly two-thirds of new drug launches miss first-year sales forecasts (McKinsey). Deloitte’s analysis of 284 U.S. launches (2012–2021) found about one-third missed expectations and more than half generated under 80% of forecast sales.
7 About one in ten launches (2020–2024) cleared $100 million in first-year revenue — roughly half the prior five-year rate. A ZS Associates retrospective of 340 launches (2008–2025) found commercial commitment raised the overperformance rate from 49% (clinical differentiation alone) to 67%.
8 An estimated 95% of enterprise AI pilots fail to deliver measurable business impact. MIT (Project NANDA), “The GenAI Divide,” 2025.
9 72% of CEOs report their boards are pressing for measurable AI outcomes, up from 61%. Dataiku, “Global AI Confessions Report,” 2026.
10 Ethan Mollick, “The Shape of AI: Jaggedness, Bottlenecks and Salients”, 2025
11 Colin Fraser
12 McKinsey posits that agents could free up 25 to 40 percent of pharma employees’ workloads. McKinsey & Company, “Reimagining life science enterprises with agentic AI”, 2025.